1. Introduction
Patients who visit dental clinics usually feel a vague fear and stress for indefinite reasons, often, these feelings are caused not only by the circumstances of the dental atmosphere—such as smell, sight, and sounds—but also due to their experiences and memories. This is related to dental attitudes and cooperation (1-4). Hence, all such senses that a patient relates to dental practices are called dental stress and, similarly, dental fear or dental anxiety (5-7).
Since patients experiencing dental stress tend to avoid these stressful situations or targets, adjusting their behavior can be one of the most important factors in successful dental treatment (8-10). Therefore, many dental staff and students are studying dental stress control in the clinic (11-13).
The impression-taking process—a dental hygiene task—is known to have a deep correlation between the proficiency of dental hygienists and the patient’s discomfort (14-17). Impression-taking is simple and common for dental staff; however, patients tend to freeze under stress. Therefore, we studied the correlation of stress and impression-taking steps, by checking patient vitals. Until now, the most commonly used research tools to measure stress index are Brief Encounter Psychosocial Stress Instrument (BEPSI), Dental Anxiety Scale (DAS), and Dental Fear Survey (DFS) (18, 19). Recently, more objective tools have been introduced to measure stress levels such as through the autonomic nervous system, and blood flow measurement. In our study, we also attempted to use uBioMacpa (BioSense Creative Co., Ltd) devices using this principle to measure dental stress (20). From the results of this study, we would like to suggest steps that patients could reduce such stress.
2. Study subjects and methods
2.1. Research subjects
Sample sizes were measured using the G*Power version 3.1 program, with an effect size of 0.5, and a significance level of 0.05. A statistical power of 0.8 and a minimum sample size required for paired t-test and correlation analysis was 128. However, given the limitations of university student research, it would be difficult to find subjects for a substantially short research period, therefore the number of participants was 33, a quarter of the preferred sample size.
The study was conducted for a week, from May 28 to June 5, 2019, and 33 subjects received explanations on the purpose, method, and stability of the study, and agreed to participate. Those vulnerable to coercion or undue influence, or lacking in decision-making skills, or those who are likely to be affected by voluntary participation decisions were excluded from the sample.
The following are the criteria for selecting research subjects.
1) Persons who are currently enrolled in university
2) Persons without seeing, hearing, smell, and communication problems
3) Persons who understand and are willing to participate in the study
4) Persons who do not use nail polish and artificial nails
2.2. Methods
2.2.1. Methods
To achieve identical conditions, all experiments were conducted on the chair unit in the Oral Hygiene Education office of Yonsei University Wonju College of Medicine.
1) Step 1: Pre-impression-taking measurement
Upon visiting the Oral Hygiene Education office, subjects received explanations on the process of the research and completed the consent form. The uBioMacpa (BioSense Creative Co., Ltd), a stress meter, was placed firmly on the left index finger in the upper right position. The stress relevant index of the subjects was recorded and measured for 2.5 minutes on the monitor of the device.
2) Step 2: During impression-taking measurement
While monitoring the subject, the researcher began to mix alginate. The process of mixing materials was intentionally made directly visible to the subject. After the mixing was complete, we placed the partial tray with alginate in the oral cavity. It was kept there until monitoring had ended; after measurements were recorded, the tray was removed.
3) Step 3: Post-impression-taking measurement
After light rinsing of the mouth, the subject’s vital signs were monitored. After 2.5 minutes of measuring, subjects again rinsed their mouths and completed the questionnaire.
2.2.2. Statistical tests
The results were analyzed using SPSS 25.0 Program (IBM Co., Armonk, NY, USA). Descriptive statistics were conducted to identify frequency, average variance, and most frequent values of the general characteristics of the study subjects.
An independent t-test or paired t-test was performed to test the normality of values obtained by measuring general characteristics and stress of the subjects.
The one-way analysis of variance ANOVA was conducted to verify the stress-relevant index and pulse rate changes were measured for three periods (pre-, during, and post- impression-taking).
3. Results
3.1. General characteristics of the participants
General characteristics of the study subjects are reported in Table 1. The common traits were age and level of education; all subjects (66.7% women and 33.3% men) were in their 20s and had university education. Further, 87.9% of the subjects had prior experience with the alginate impression-taking process, and 12.1% did not (Table 1).

3.2. Measurement of stress-related index by alginate impression-taking steps
We measured the stress-related index during three steps (pre-, during, and post- impression-taking) to determine when the subject felt most stressed in the alginate impression process. Values of standard deviation of all internals (SDNN), square root of the mean of the sum of the squares of differences between adjacent NN intervals (RMSSD), and High Frequency (HF) represent strong indicators that provide information about the stability of the cardiovascular system and the ability of the autonomic nervous system to control the human body. All three indicators showed a tendency for the index to rise during the impression-taking process, and decline after it was completed (Table 2).

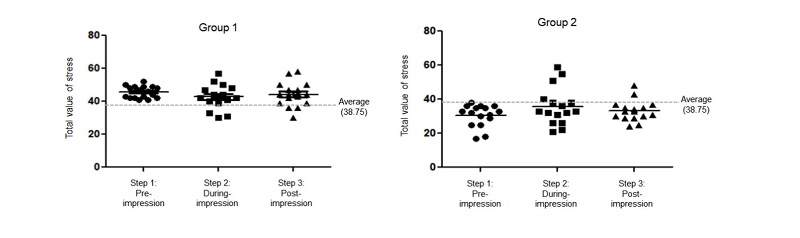
3.3. Comparison of the continuity of total value of stress
We compared how the total value of stress measured while “pre-impression-taking” (Step 1) relates to the values of “during and post impression-taking” (Steps 2 and 3). To this end, we divided participants into two groups based on the average value of the total value of stress (38.75), measured in Step 1. The high-value group was named Group 1, and the low-value group was named Group 2. As seen in Figure 1, for Group 1, 76.5% and 82.3% of subjects in Step 2 and Step 3, respectively, presented a series of stress values that were higher than the average. Group 2, which exhibited lower average stress values, also continuously presented stress values in Steps 2 and 3 of 75% and 87.5%, respectively, and were below the average. Both were statistically significant correlations (p<0.01).
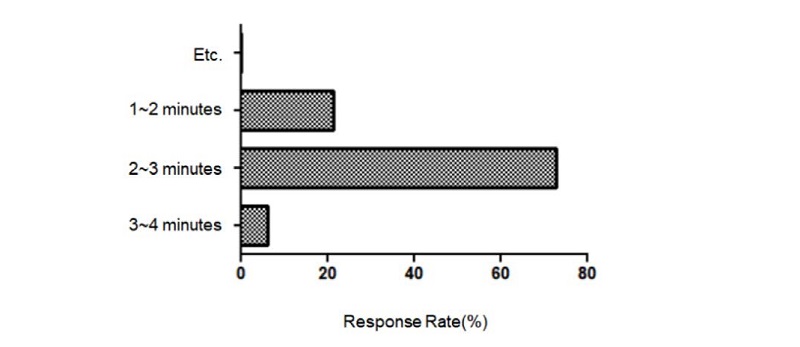
3.4. Results of questionnaires on discomfort in the alginate impression-taking process
Results of questionnaires on satisfaction with alginate impression-taking revealed that 6.1% of participants were dissatisfied, 30.3% were neither satisfied nor dissatisfied, 39.4% were mostly satisfied, and 24.2% were very satisfied (Figure 2). The subjects reported poor smell, touch, and time for taking the impression as reasons for dissatisfaction. Among these, time required to take impressions is directly related to the proficiency of dental hygienists. In all, it is reported that two to three minutes was the most appropriate duration for alginate impression-taking with 72.7% response (Figure 3).

4. Discussions
Alginate impression-taking is a common and basic task performed by dental hygienists. However, there are very few studies about the discomfort or fear that patients experience during the process. Therefore, by quantifying the stress index in this study, we tried to determine how alginate impression-taking influences stress. We also sought to identify factors contributing to dental stress and find ways to increase cooperation in patients’ dental care by lowering the overall stress index that can occur in dentistry.
To this end, we confirmed a method to measure stress through the autonomic nervous system. We identified changes in SDNN, which indicates activity of the entire autonomic nerve, RMSSD, and HF, as well as activity balance of the parasympathetic nerve (Table 2). This allows us to understand that alginate impression-taking changes the activity of the autonomic nerve when it acts as a stress factor for the patient. This, in particular, means increasing activity of the parasympathetic nerve.
According to the study, the stress index showed highest values during the actual taking of the alginate impression (Step 2) due to the use of dental materials. In addition, the unfamiliar taste and texture of alginate may create fear within the patient.
Furthermore, low values of HF and RMSSD, which represent anger, anxiety, and fear, were lowest after impression-taking (Step 3). This means that subjects felt most uncomfortable after the process was completed. Therefore, it is important for dental hygienists to make efforts to reduce the discomfort even after the impression has been taken.
The stress index and HF index were both second-highest while pre-impression-taking. It is considered necessary for dental hygienists to comprehensively brief patients before commencing on dental work.
Therefore, measures to reduce patients’ inconvenience in impression-taking include improving alginate touch and taste, as well as improving education and dental hygienic service of dental hygienists to reduce stress in patients before and after the process.
In this study, we tried to determine the effect on the stress index when taking alginate impressions. However, due to characteristics of student research, a majority of the subjects were limited to dental hygiene students because of the short duration of the study and difficulties in recruiting a sufficient sample. It was also challenging to control the behavior of the subjects, in addition to environmental control.
Based on this study’s results, it is believed that continuous research should be conducted to suggest a way to alleviate dental stress in impression-taking.
5. Conclusions
This study was conducted on a period-by-time basis using uBioMacpa to determine the effect of alginate impression-taking on the dental stress index in some university students, and concluded that:
1. The most stressful step in the alginate impression-taking process was during the actual taking of the impression, followed by the pre- and post- steps.
2. The more likely the subject was considered to be nervous (total value of stress is 38.75 or higher) at the pre-impression-taking step, the higher the likelihood of stress being increased or maintained at the during and post stages of impression-taking.
3. From a perspective of dental hygienists implementing anti-stress techniques, this study can contribute toward bringing relief to patients’ dental stress by lowering their tension before alginate impression-taking.
